Usefulness of the article : The COVID-19 epidemic is likely to significantly increase poverty around the world. The poorest populations are in fact doubly exposed. From a health perspective, they are at greater risk of contracting the virus and developing a severe form of the disease. From an economic standpoint, the pandemic is likely to have a greater impact on the incomes and living standards of the poorest populations. The current pandemic therefore risks exacerbating existing socioeconomic inequalities.
Summary:
· The COVID-19 epidemic is likely to lead to a sharp increase in poverty;
· The poorest populations are likely to suffer the hardest from the impacts of this epidemic;
· They are indeed more exposed to health and economic risks.


The crisis we are currently experiencing with the COVID-19 epidemic is above all a global health crisis, with nearly 150,000 deaths worldwide (figures from mid-April 2020). The current priority is obviously to deal with the situation by saving as many lives as possible, ensuring that our healthcare systems are able to cope with the influx of patients.
It is also necessary to recognize that COVID-19 will have short- and long-term economic and social consequences. As a result of lockdown measures, the economy has come to a standstill in many sectors, leading to a sharp decline in activity. On April 9, 2020, INSEE estimated that the loss of activity in France was nearly 35%. It is therefore highly likely that this epidemic will have an impact on household living standards and poverty around the world.
While the virus can infect anyone and does not discriminate between social classes, there are many reasons to believe that certain people, the most vulnerable and disadvantaged, are more likely not only to be affected by the virus but also to suffer economically. The epidemic is therefore likely to affect the most marginalized populations first and foremost, reinforcing existing socio-economic inequalities.
COVID-19 and poverty: some estimates
To date, the data available to us is preliminary and the future remains uncertain. It will therefore need to be supplemented by more in-depth analysis in the future. Nevertheless, a recent article published by UNU-WIDER (United Nations University World Institute of Development Economic Research)[1] has attempted to measure the short-term effect of COVID-19 on monetary poverty. The authors simulated three scenarios of varying severity: a 5%, 10%, and 20% decline in household consumption or per capita income. In all cases, estimates show that global poverty will increase for the first time since 1990. The most extreme scenario shows that the number of people living in monetary poverty could increase by half a million compared to 2018[2]. Certain regions, such as sub-Saharan Africa and South Asia, would be particularly affected (Figure 1). These estimates are in line with those of the International Labor Organization, which highlights that there will be 9 to 35 million new working poor in developing countries in 2020. Similarly, Vos, Martin, and Laborde have estimated that a 1 percentage point decline in global GDP could lead to an increase in poverty, with 14 to 22 million more people living on less than $1.90 per day[4]. All these studies therefore show that the current epidemic could undermine the fight against poverty. This risks calling into question the possibility of achieving the Sustainable Development Goals by 2030, particularly thefirst goal, which aims to eradicate extreme poverty worldwide.
Figure 1: Percentage of individuals living on less than $3.20 per day in 2015, assuming a 20% contraction in income
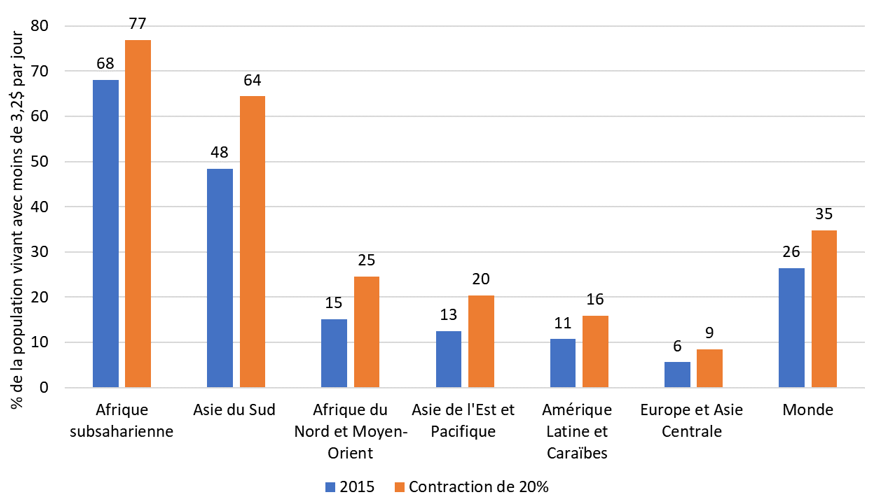
Source: Author using data from A. Sumner, C. Hoy, and E. Ortiz-Juarez. (2020). Estimates of the Impact of COVID-19 on Global Poverty. UNU-WIDER: Helsinki
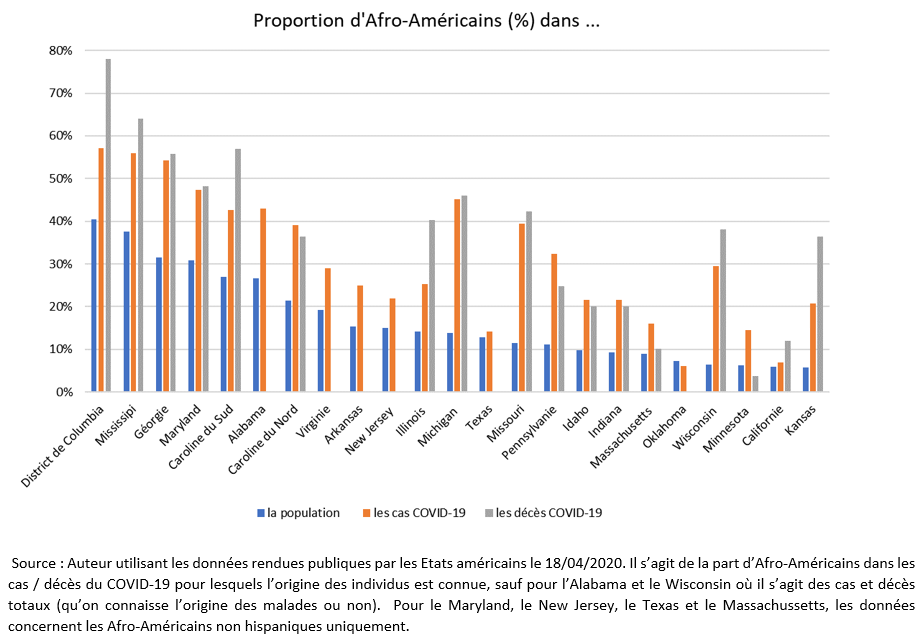
Initial evidence suggests that within countries, the most disadvantaged populations are particularly affected by the COVID-19 epidemic. This is the case in the United States, where preliminary data show that African American populations, which are often more disadvantaged, are more affected by the virus. Although not all states have yet provided detailed statistics, 30% of reported COVID-19 cases involve African Americans, who represent only 13% of the total population. This disparity is found in many US states (Figure 2). For example, in Michigan, nearly half of COVID-19 cases and deaths are among African Americans, even though they represent only 14% of the state’s population.
In France, some data also suggest that COVID-19 affects disadvantaged areas more on average. For example, the epidemic is raging in Seine-Saint-Denis, the poorest department in metropolitan France, with twice as many deaths between March1 and April 6, 2020, as in 2019 (INSEE). This excess mortality (+102%) is higher than in other departments bordering Paris (+99% in Hauts-de-Seine and +78% in Val-de-Marne). Once again, these are partial and preliminary data. Furthermore, what we are measuring here is primarily a correlation and not a causality.
Arevulnerable populations at greater risk?
If the COVID-19 epidemic is likely to increase poverty, it is primarily because the most marginalized and vulnerable populations are more exposed to the health and economic risks associated with the virus. Not only are these populations more likely to be affected by the virus—and to contract severe forms of it—but they are also likely to suffer more severely from the economic consequences of this crisis.
Greater exposure to health risks
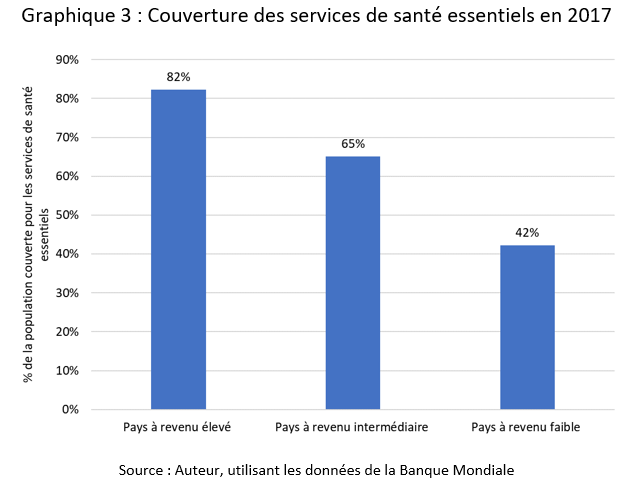
First, the most disadvantaged populations are more likely to be exposed to the disease. This is because the poorest and most marginalized often have less access to healthcare. These populations are therefore less likely to be tested and treated after contracting the disease. This is particularly true in countries where access to healthcare is not universal and can be costly, sometimes prohibitively so for the most disadvantaged. In the United States, for example, in 2018, 14% of individuals in the poorest households were not covered by health insurance, compared to 3% of individuals in the richest households. In some countries, particularly the poorest ones, healthcare systems are often failing due to corruption, lack of infrastructure, human and material resources, discriminatory practices, etc. In these countries, a significant proportion of the population does not have access to essential health services (Figure 3). This health situation may explain why poverty is likely to increase sharply in developing countries affected by the epidemic. These countries are unable to cope with the situation, and the populations most likely to suffer are the poorest.
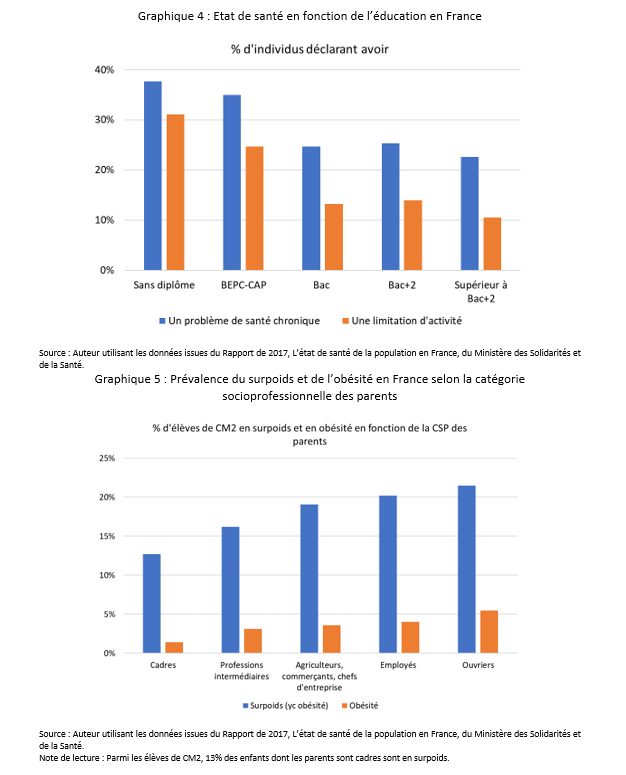
Even in countries with universal healthcare systems, inequalities persist and, in reality, not everyone has access to healthcare on the same terms or enjoys equal health outcomes. In France, for example, there is a 6.8-year gap in life expectancy at age 30 between the most educated and least educated men (OECD). In 2014, 39% of the poorest individuals reported having to forego healthcare for financial reasons, compared with 13% of the richest[7]. In fact, disadvantaged populations are in poorer health and are more likely to have chronic diseases that can be comorbidities and promote the development of severe forms of COVID-19 (Figure 4). Young people from disadvantaged backgrounds, for example, are more likely to be overweight or obese, which are aggravating factors in the event of COVID-19 infection (Figure 5).
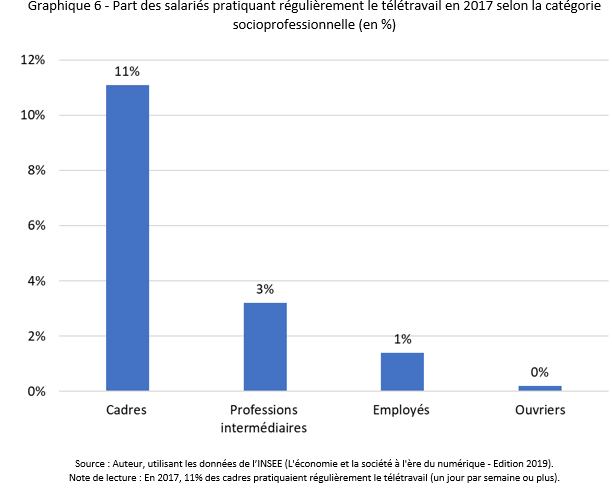
Disadvantaged individuals are overrepresented in economic sectors considered essential during this period of lockdown (transportation and delivery, food, home help, etc.). These jobs are characterized by close contact with others, which makes social distancing difficult and increases exposure to the virus. Not all jobs are equally suited to teleworking. Many individuals, often those in the most disadvantaged socio-professional categories, are unable to telework (Figure 6). Even when their jobs are not considered essential, the most disadvantaged individuals, who have no savings, often have no choice but to continue working, putting themselves on the front line in the fight against the virus. This is especially true in countries where social security systems are non-existent or inadequate and where these people must choose between working and risking infection, or not working and losing their financial resources.
Finally, the living conditions of poor people may also explain why they are more exposed to the health risks associated with COVID-19. These populations are more likely to live in smaller, more crowded homes, which makes social distancing difficult and increases the risk of infection. In 2013, 30% of the poorest households lived in overcrowded housing, compared with 2% of the richest households. In such housing, social distancing is not only more difficult to practice but also more difficult to endure (consequences for mental health). Lockdown therefore risks deteriorating the quality of life and health of the most disadvantaged individuals.
Greater exposure to economic risk
Not only are the most disadvantaged people more exposed to the health risks posed by COVID-19, but the economic consequences are also more disastrous for them. First of all, these populations often hold precarious and vulnerable jobs (temporary work, fixed-term contracts, piecework, informal employment). However, these jobs offer less protection and are the first to be affected by layoffs. In France, for example, 12.5% of people in fixed-term employment in 2017 found themselves unemployed a year later, compared with 1.6% of those on permanent contracts.
In low-income countries, this situation is particularly worrying, as many individuals work in the informal sector (81% of total non-agricultural employment). However, these jobs are generally precarious, offer little protection, and are particularly vulnerable to economic shocks. Furthermore, as mentioned above, many people in the poorest socioeconomic classes are unable to work from home (e.g., those in manual occupations) and are therefore likely to see their incomes fall sharply as a result of lockdown measures, particularly in countries where social protection is weak or non-existent. These populations are therefore likely to bear the brunt of the loss of income caused by the epidemic, especially since they generally do not have savings to cope with such a loss of income.
Lockdown measures are also placing new costs on households (excessive consumption of heating and electricity, increased food expenditure due to the closure of canteens, etc.), which can be a real burden for the most vulnerable.
Finally, in the long term, lockdown and social distancing measures are likely to weigh more heavily on the most vulnerable households. With schools closed in many countries, learning is taking place remotely, which is particularly difficult for children from disadvantaged backgrounds who do not have the material resources (good internet connection, available computer, quiet place to study) or human resources (help, parental supervision) necessary to cope with this situation. The epidemic is therefore likely to exacerbate socioeconomic inequalities in education.
A concrete example: migrants
Immigrants are among the most vulnerable populations during this pandemic, as highlighted by the Institut Convergences Migrations in April 2020[11]. These populations combine many characteristics that put them at greater risk. Many encounter difficulties in accessing information and understanding the healthcare system and preventive measures (partial language proficiency, complexity of healthcare systems, lower levels of education). Some migrant groups also have poorer health[12] and may suffer from chronic diseases (overweight, diabetes), which are comorbidity factors that can lead to severe forms of COVID-19. They often have less access to the healthcare system and make less use of healthcare services[13], have more vulnerable jobs, and live in precarious[14] or overcrowded housing that makes confinement difficult (hostels, shelters, camps, etc.). In these often unsanitary housing conditions (lack of access to water, soap, etc.), where it is difficult to avoid close contact with others, migrants are unable to implement the recommended protective measures. In addition, migrants often find themselves without any income as a result of lockdown measures and in many cases are unable to benefit from government aid aimed at compensating for loss of income. In India, for example, the government has set up an aid system for Indian citizens. Following the announcement of lockdown on March 25, Indians who had migrated to urban centers to find work found themselves stuck, unable to return home due to a lack of transportation, and many were therefore unable to claim their right to this aid.
Conclusion
Initial estimates suggest that the COVID-19 pandemic is likely to lead to a sharp increase in poverty. It is highly likely that the most disadvantaged populations will be hardest hit due to their greater exposure to health and economic risks.
It is therefore important to recognize that COVID-19 is likely to exacerbate inequalities and increase poverty. Countries must be aware of this and focus their efforts on the most isolated, marginalized, and vulnerable populations (the poor, informal and precarious workers, migrants, homeless people, etc.) to ensure that they receive financial and human assistance to cope with the epidemic. In the long term, the current crisis will be an opportunity to rethink health and social protection systems to ensure greater equity.
Governments must also not forget their commitment to fighting poverty. There is a real fear that once the health crisis is over, the economic consequences will be felt, notably in the form of increased public debt as a result of the measures taken by governments. To restore public finances, countries may be tempted to put the fight against poverty on the back burner, for example by reducing official development assistance, which would undoubtedly have very serious negative consequences. One option would be to cancel part of the debt service of developing countries maturing in 2020 to enable them to free up resources that could be mobilized in the fight against COVID-19. For the time being, the G7 has opted not for cancellation but for suspension.
[1]A. Sumner, C. Hoy, and E. Ortiz-Juarez. (2020). Estimates of the Impact of COVID-19 on Global Poverty. UNU-WIDER: Helsinki. Downloadable here: https://www.wider.unu.edu/sites/default/files/Publications/Working-paper/PDF/wp2020-43.pdf
[2] These estimates vary from 419 to 581 million depending on the poverty line chosen (USD 1.9, USD 3.2, or USD 5.5 per day).
[3] The working poor are defined here as those earning less than $3.2 per day. ILO (2020) “COVID-19 and the world of work: impact and policy responses.” Downloadable here: https://www.ilo.org/wcmsp5/groups/public/—dgreports/—dcomm/documents/briefingnote/wcms_738753.pdf
[4]Vos, R., W. Martin, and D. Laborde. (2020). “How much will global poverty increase because of COVID-19?” Downloadable here: https://www.ifpri.org/blog/how-much-will-global-poverty-increase-because-covid-19
[5] https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html and https://www.census.gov/quickfacts/fact/table/US/PST045219
[6]Health Insurance Coverage in the United States: 2018. The poorest households are those with an annual income of less than $25,000, and the richest are those with an annual income of more than $150,000.
[7] Ministry of Solidarity and Health. The state of health of the population in France – 2017 REPORT
[8] Data from the Observatory of Inequalities. Households are classified by income decile. Overcrowded housing is defined by INSEE as not including at least: a living room, one bedroom for couples, one for single people aged 19 or over, one for two children (if they are of the same sex or under the age of 7) or one bedroom per child.
[9] INSEE. Employment, unemployment, and income from work. 2019 edition.
[10] Statistics obtained from World Bank data. Average informal employment rate in non-agricultural employment in the 15 low-income countries for which data is available between 2010 and 2019.
[11] CONVERGENCES MIGRATIONS Institute. De Facto. April 18, 2020. « Migrants in the epidemic: a time of cumulative hardship. » Downloadable here: http://icmigrations.fr/defacto/defacto-018/
[12] Berchet, C., & Jusot, F. (2012). Health status and use of healthcare by immigrants in France: a review of the literature (No. hal-01593735).
[13] Berchet, C., & Jusot, F. (2012). Health status and use of healthcare by immigrants in France: a review of the literature (No. hal-01593735).
[14] Living conditions – Immigrants – INSEE References – 2012 edition